
2022 Blog Entries
12/12/2022
Finally have a quick minute to sit back and admire this years accomplishments. None of this could have happened without the support of various vendors, AHS's imaging and leadership staff, and the
instilled confidence from our managing partners/owners.
1.Weathered the 'great resignation' storm. Bittersweet in the sense we did lose some talent, however were extremely fortunate to not just attract quality
new-hires, but retained quite a number of our tenured staff that continue to align with AHS culture and core values.
2. Tackling the pharmaceutical, iodinated contrast, and general supplies shortage. Between backordered tubing, saline, lidocaine, fentanyl, invasive procedural
sheaths and catheters, blood-drawing vacutainer tubes - this still remains a constant challenge albeit strategically expanding our list of medical supplies distributors to fill in various inventory
gaps has worked out fairly well.
3. Moved our 64 slice CT to our Johns Creek facility, then installed a 128 slice CT at our Tucker facility.
4. Setup our new local EESI PAC's server which acts as a centralized repository for most of our imaging modalities.
5. Integrated Biotricity's remote cardiac all-in-one monitoring devices to all AHS locations.
6. Expanded our nuclear cardiac amyloid imaging services to both our Tucker and Johns Creek locations.
7. Upgraded all eight AHS locations to newer GE Echopac versions.
8. Ramping up vascular procedures at our newest outpatient based lab in Johns Creek.
9. With having two full-time CT labs, we've essentially doubled our CT volumes with our coronary CTA's reaching a milestone of ~45/50 per
month.
10. Integrated Cleerly's AI assisted plaque morphology coronary CTA analysis services at both the Tucker and Johns Creek
locations.
11. Expand our Podiatry (Atlanta Podiatry Specialists) services to a number of AHS locations.
12. Successful reaccreditation with ICAVL, ICAEL, and ACR.
Goals for 2023:
1. Ramp up our vascular procedures at Johns Creek's OBL.
2. Explore bringing our coronary CTA interpretations in-house.
3. Continue to expand nuclear amyloid imaging to other AHS locations.
4. Explore software enhancements to our 64/128 slice CT systems that have the potential to improve the quality of our coronary
CTA's.
5. Integrate generic Lexiscan - if commercially available.
6. Explore strategic alliances to challenge Georgia's CON laws.
10/15/2022
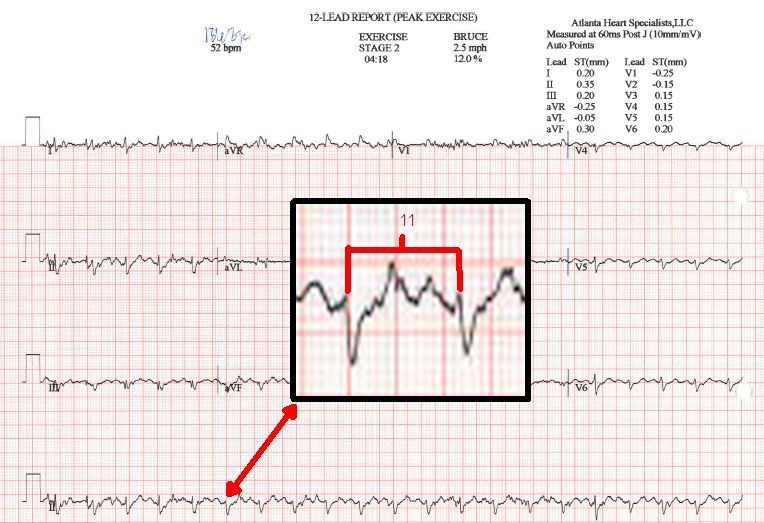
Knowing how to manually calculate a patients heart-rate off an EKG is essential when performing certain exams (ie, MPI, stress test) on the
treadmill.
In this case, the stress system read the patients heart-rate as 0 bpm due to diffuse, poor QRS voltage. Took another 12 lead, and then it read 52 bpm, which is
completely erroneous just by looking at the R-R interval itself.
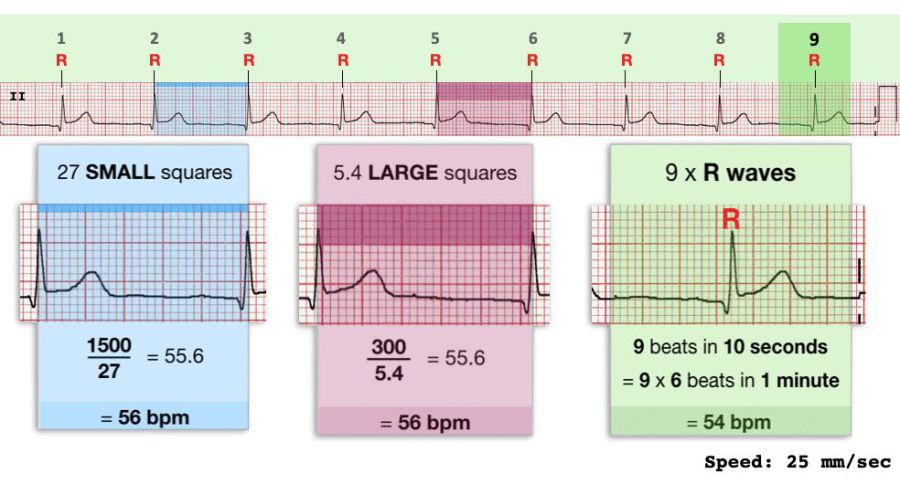
There are three ways of calculating the heart-rate, shown in the attached slide. In this particular instance, I counted 11 small boxes giving us a heart-rate
of 136. Patient was 87 years old, so 220-87 gives us their 100%MPHR of 133bpm. Dividing 136/133 gives us 102% as their max achieved heart-rate, well above the desired 85%.

9/25/2022
Very detailed presentation from KaufmanHall depicting an ominous financial outlook for our healthcare system.
Congress needs to be taking this emerging landscape very seriously.
Removing post-pandemic funding along with proposed Medicare/Medicaid reimbursement cuts has the potential to cripple an already fractured
infrastructure.
Key takeaways:
• Projections for the entirety of 2022 indicate an increase in hospitals with negative margins, to 53%.
• Expenses are projected to increase throughout 2022, leading to an increase of nearly $135 billion over 2021 levels.
• Labor expenses are projected to rise $86 billion in 2022, while non-labor expenses are projected to increase by $49 billion.
• Contract labor expenses remain nearly 500% higher than pre-pandemic levels.
• All expense categories are projected to remain approximately 20-25% above pre-pandemic levels, with drug and supplies increasing the
most.
Adobe Acrobat document [912.7 KB]
9/11/2022
Over the years I've been fairly vocal on how the general publics perception on radiation is misguided due to antiquated, dispelled data.
Back in February 2017 renowned medical physicist Jeffry A. Siegel dispelled the 70 year old hypothesis via the Journal of Nuclear Medicine that exposure to
medical radiation could increase ones risk of cancer. In fact, he suggested it more likely helps prevent it (radiation hormesis).
Then in March 2017 JNM issue, like ripples in a pond, numerous professionals in the field were siding with Dr.Siegel. This issue alone has an astonishing
five letters to the editor referencing his original article.
The consensus thus far weighs in favor of a complete overhaul which some argue "would likely result in the elimination of many government jobs and
significantly reduce the budget of the federal and state regulatory agencies."
More and more studies, like the one referenced below (albeit somewhat limited), are continuing to challenge the status quo surrounding medical radiation to
hopefully reshape what can be best described as highly controversial.
Adobe Acrobat document [881.8 KB]
9/7/2022
Quick question: what does flurpiridaz and TruGreen have in common? *Skip to below.
For those in the field of nuclear cardiology, it's
very exciting to see the data derived from the phase III Aurora trial for F18-flurpiridaz. Once the FDA review process is complete, hopefully we'll see it
commercially available mid-late 2023.
*Flurpiridaz is a chemical analog of pyridaben, a well established insecticide and acaricide. At certain doses, the EPA has documented studies on its
neurotoxicity profile, as well as it's category III toxicity classification.
Now, did anyone happen to notice the safety profile during this trial? Out of the 604 enrolled patients, there were 25 observed adverse events, with 14 of them
being 'serious,'
Could these 'serious' reactions have any relation to pyridaben's documented neurotoxicity profile?
6/15/2022
Very unique case study on how intravenous iron treatments can lead to a false-positive finding on cardiac amyloid scans using
Tc99m-HMDP.
Curious to know if this would be applicable to Tc99m-PYP?
6/7/2022
I can think of three companies that won't be happy with these FFR-CT findings.
Wonder how the ACC/AHA will respond considering their latest addition of FFR-CT into chest-pain guidelines designates it as a key component of their
recommended evaluation algorithms.
"Researchers completed a retrospective review of more than 1,100 coronary CT angiography exams and found that FFR-CT did not have an clinical effect over the
Coronary Artery Disease Reporting and Data System for assessing CAD and that "the routine use of FFR-CT in CAD-RADS 2-4 [patients] gives reduced accuracy and specificity without a significant
increase in sensitivity.""
5/20/2022
Will molecular imaging have a key role in better understanding the long-term effects of COVID-19 on the brain? This JNM article provides a preliminary suggestion on the possible future use of PET and SPECT to investigate central nervous system manifestations of COVID-19.
Adobe Acrobat document [897.3 KB]
4/20/2022
The cracks are officially forming. A number of major hospital chains have filed massive quarterly losses attributing them to costs of agency staff, wage
increases and retention, as well as supply costs.
One suggested solution is to hold the insurance companies partly responsible by having them fit the bill for the added costs. However, that would ultimately be
passed down to the consumer in the form of increased premiums.
It will be interesting to see how healthcare leadership organizations deal with these massive financial rifts.
CommonSpirit posts $591M quarterly operating loss
https://lnkd.in/gsU8veY2
Advocate Aurora posts $253M net loss in Q1
https://lnkd.in/gYRjU26u
Providence's operating loss hits $510M in Q1
https://lnkd.in/gbiA4XqK
Mass General Brigham posts $867M quarterly net loss
https://lnkd.in/g9PtSQsx
Kaiser Permanente faces $961M net loss in Q1 2022 due to high expenses, poor investments
4/12/2022
Hot off the press! A fantastic summation of things to come in the world of nuclear cardiology.
Wanted to also point out the significance of F-18's Flurpiridaz's myocardial extraction (Figure 2) when compared to other FDA approved perfusion
agents.
The question now is: when will Flurpiridaz be commercially available and will its assigned reimbursement be pragmatic?
Adobe Acrobat document [1.4 MB]
4/1/2022
With the saline shortage in full effect, I put in a request with the FDA to consider a number of manufacturers products to be added onto their 'Extended Use'
list, which can be found here.
The current list is unfortunately underwhelming, however if enough requests are made to both the FDA and saline manufacturers, the potential is there to the
extend the shelf-life of necessary pharmaceuticals.
More information on the saline shortage can be found below:
https://lnkd.in/dHq8fMbt
https://lnkd.in/d7hEiEF7
3/15/2022
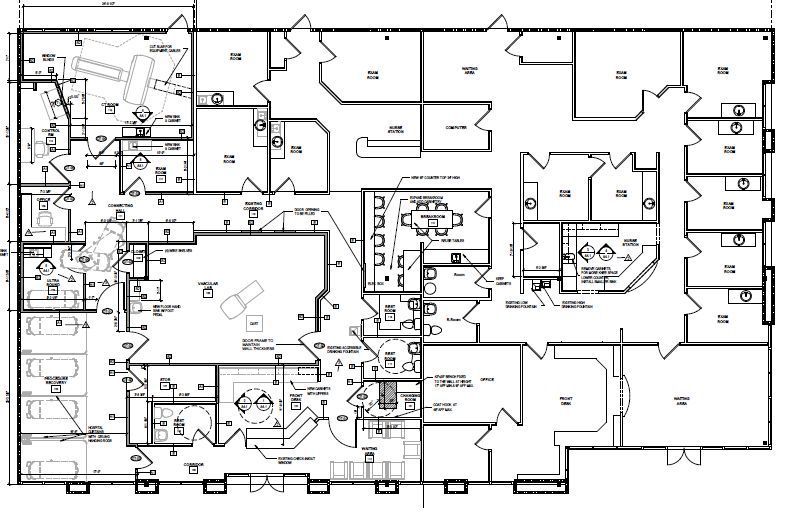
After a long 16 months, and having sent out 1000+ emails to equipment vendors, service engineers, application specialists, lenders, architectural firms,
structural/electrical engineers, general contractors, electricians, municipalities, Georgia's Certificate of Need program, legal counseling, and physicists - our Johns Creek expansion space which now
offers 64 slice CT imaging, vascular related imaging, and interventions - is now complete - AND our Tucker facility is sporting a GE 128 slice Optima 660 CT scanner!
This couldn't have gone any smoother thanks to the following companies:
Schoppman Company, Gary B. Coursey & Associates, Barrett Woodyard & Associates, GE, Alphasource, Brown's Medical Imaging, United Community Bank,
Siemens Financial, Goldstar Electric, Ray & Gregory LLC, Alliance Medical Physics, and Block Imaging.

3/3/2022
So, I guess I'll pitch the icebreaker: where's the news coverage on how these healthcare supply chain issues are completely disrupting patient care in the
private practice setting?
Today I was instructed by our distributor (in the Fortune 500) that the bulk of our locations are only eligible for one bag of saline - per
month.
Keep in mind we are one of the largest privately owned cardiology practices in Georgia with over 160 staff, and nine locations. Between the out patient visits
and diagnostic testing, some of them see hundreds of patients a day.
How are we to treat hypovolemic/dehydrated/POTS patients by saving them a very expensive trip to the ER? How are we to dilute our pharmaceuticals? How do we
flush our patient tubing? How are we to perform our outpatient atherectomy procedures? How are we to perform diagnostic testing that require line-clearing boluses?
My question is: what and how are the major GPO's, and medical distributors, doing to level the supply procurement process between massive hospital chains and
private practices?
2/25/2022
Any Imaging Directors/Managers that routinely interact with Georgia's Radioactive Materials Division, please be advised they have now started enforcing the
below rule:
391-3-17-.05(30)(b)(1) states, A licensee shall ensure that the survey instruments used to show compliance with Rule .05 and Rule .03 of this Chapter, have
been calibrated before first use, annually, and following any repair that will affect the calibration. Calibrate all required scale readings up to 10 millisievert (1,000 mrem) per hour with a
radiation source.
Out of all of our radiation detection equipment, we're now having to replace two Ludlum 3 GM's because they don't meet this requirement as they max out at
x100. Which begs the question: when was the last time anyone in your nuclear medicine department had to use the x1000 setting on a GM meter (hoping no one)?
2/8/2022
For those of you impacted by the Tc99m-PYP shortage, please be advised ASNC is recommending Tc99m-HMDP as a suitable alternative. Silver-lining is that HMDP might come at a lower cost than your
PYP!
Adobe Acrobat document [420.3 KB]
2/1/2022
ASNC released their formal stance on current AHA/ACC Chest Pain Guidelines which gave FFR-CT an inappropriately large role - and rightly so. The technology is
cost-prohibitive, proprietary to one vendor, and lacks accessibility. https://rdcu.be/cHKSA
"Despite ASNC’s policy of collaboration and inclusivity and its long track record of collaborative guideline development, we are unable to endorse the current
AHA/ACC Guideline for the Evaluation and Diagnosis of Chest Pain. The lack of balance in the document’s presentation of the science on FFR-CT and its inappropriately prominent endorsement detract
from ASNC’s core principle of patient first imaging. We believe that the document fails to provide unbiased guidance to healthcare professionals on the optimal evaluation of patients with chest
pain."
1/4/2022
This study is both fascinating and chilling. And what's up with Colorado's lack of available data? Regarding Uranium, really not that surprising. If you're
really bored, check out this link and compare these documented Uranium concentrations to their Terrestrial Radiation map.